Hello everyone,
There is a growing number of older adults in America.
Currently, it is estimated that there are about 40 million older adults. That
number is expected to grow to over 92 million by 2060. A 2012 study by the US Census Bureau indicates the number of people over
65 will outnumber youth under 18 by 2056.5 Every year the number of older adults living
in an institution offering at least one supportive service (nursing care, meal
preparation, cleaning service etc.) increases. Between 2001 and 2012
showed a 1% increase in institutionalized older adults 65-74 years of age. The rates increased with age to 3% and 11% for
older adults 75-84 and over 85 respectively6. Furthermore, the
average person age 65 lives an additional 19 years. Men age 85 may live up to 6
years longer and women of same age another 7 years 1.
Health, Exercise, and Aging
 |
| © Robert Kneschke | Dreamstime.com |
There are some older adults whom cannot perform these
recommended guidelines because of some chronic conditions. It is suggested that
these individuals stay as physically active as possible. Older adults should concentrate on exercises
that support balance to reduce the risk of falls. All older adults should
collaborate with their doctor and fitness professional to establish a base
fitness level. Together an effective activity program can be created and help
the older adult understand how chronic conditions may affect their goals.
Regular exercise can help older adults retain daily
independence. Programs designed to speed up reaction times are invaluable in
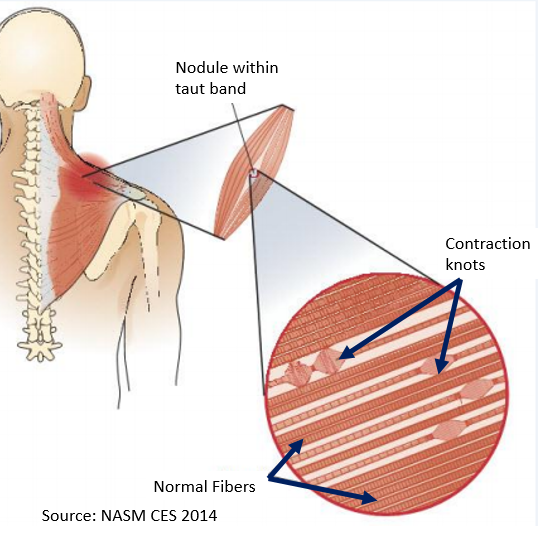
adults over 60. The aging process brings about changes in the body. Many suffer
from sarcopenic obesity. This is the chronic loss of muscle while
simultaneously increasing fat mass. Sarcopenic obesity increases the chances of
metabolic diseases in older adults. The loss of muscle is a primary contributor
to increased risk of falling. Sadly, the fear of falling is just as damaging as
the actual fall. The psychological impact of a fall encourages older adults to
become less active thereby perpetuating the decrease in physical ability.

It is accepted that the ankles are primarily responsible for
posture and balance. Research suggests that exercises as simple as heel raise with alternating arm-reach can help increase ankle stability2. Physical
activity may help older adults retain higher levels of mobility by increasing
neuromuscular sensitivity3. Regular physical activity and exercise
can promote increased release of neurotransmitters like dopamine,
norepinephrine, and acetylcholine used by the central nervous system and
peripheral nervous system. Incorporating a
aerobic/strength training combination is best to improve overall behavioral
responsiveness.
In conclusion, incorporating
an exercise program geared to promote aerobic fitness, strength and the ability
to maintain activities of daily living
are desirable. 85% of older adults suffer from at least one chronic condition
and nearly 57% of national health care costs4. Taking small steps to
regain independence and slow age-related
chronic conditions can significantly reduce the $13,000.00 per person annual
health care cost. We are all going to get older. The question is how are we planning to spend that time?
Stay healthy everyone,
-Reuben

References
1.
Academy of Nutrition and Dietetics. (2012, August).
Position of the Academy of Nutrition and Dietetics: Food and Nutrition for
Older Adults: Promoting Health and Wellness. Journal of the Academy of
Nutrition and Dietetics, 112(8), 1255-1277.
doi:10.1016/j.jand.2012.06.015
2.
Fujiwara, K.,
Toyama, H., Asai, H., Yaguchi, C., Irei, M., Naka, M., & Kaida, C. (2011,
September). Effects of Regular Heel Raise Training aimed at the Soleus Muscle
on Dynamic Balance Associated with Arm Movement in Elderly Women. Journal
of Strength and Conditioning Research, 25(9), 2605-2615. Retrieved from
www.nsca-jscr.org
3.
National
Academy of Sports Medicine. (2012). Senior Fitness Specialist Manual.
4.
Office of
Disease Prevention and Health Promotion. (2015). Scientific Report of the
2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary
of Health and Human Services and the Secretary of Agriculture. Retrieved
from www.health.gov
5.
U.S. Census
Bureau. (2012, December 12). United States Census Bureau. Retrieved
September 24, 2015, from U.S. Census Bureau Projections Show a Slower
Growing, Older, More Diverse Nation a Half Century from Now:
http://www.census.gov/newsroom/releases/archives/population/cb12-243.html
6.
U.S. Department
of Health and Human Services. (2012). A Profile of Older Americans: 2012.
Administration on Aging.